Coracobrachialis Muscle
| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Coracobrachialis | Coracoid process | Humerus (in line with crest of lesser tubercle) | Musculocutaneous n. C5 - C7 |
GHJ: Flexion, Adduction, IR |
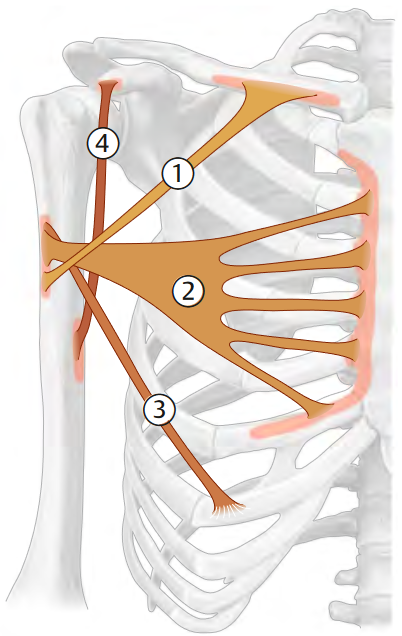
Origin
Insertion
The coracobrachialis inserts on the medial surface of the middle 1/3 of Humerus (in line with crest of lesser tubercle)1
Innervation
The musculocutaneous n.1 and (C51, C61, C71) give innervation to the coracobrachialis muscle.
Musculocutaneous n. innervates the muscle as it passes through the muscle6.
Action
Since the coracobrachialis originates from the scapula and inserts on the humerus, it primarily affects the glenohumeral joint (GHJ). The coracobrachialis performs
When looking at the shoulder as a whole, the coracobrachialis assists with the first 0-60° of shouulder flexion/elevation since this primarily involves the glenohumeral joint6.
The coracobrachialis functions to support the anterior shoulder7.
Function
Coracobrachialis serves as a secondary flexor and adductor of the shoulder8.
The coracobrachialis is usually recruitted when:
Myofascial Functional Unit
The coracobrachialis and pectoralis minor both have insertions on the coracoid process, which creates a myofascial line9. When the arm is relaxed by one’s side since the pec minor and coracobrachialis fascial lines run in two different directions, thus the line is inactive9. However, when shoulder is brought into overhead flexion (i.e. tennis serve or hanging from a bar)9.
This connection will combine with other myofascial units to form the Deep front of arm line and the Deep Front Line9.
Dysfunction
- Since the musculocutaneous n. passes through the muscle belly, coracobrachialis dysfunction can entrap the nerve and create neurological symptoms6.
Pathologies
Palpation
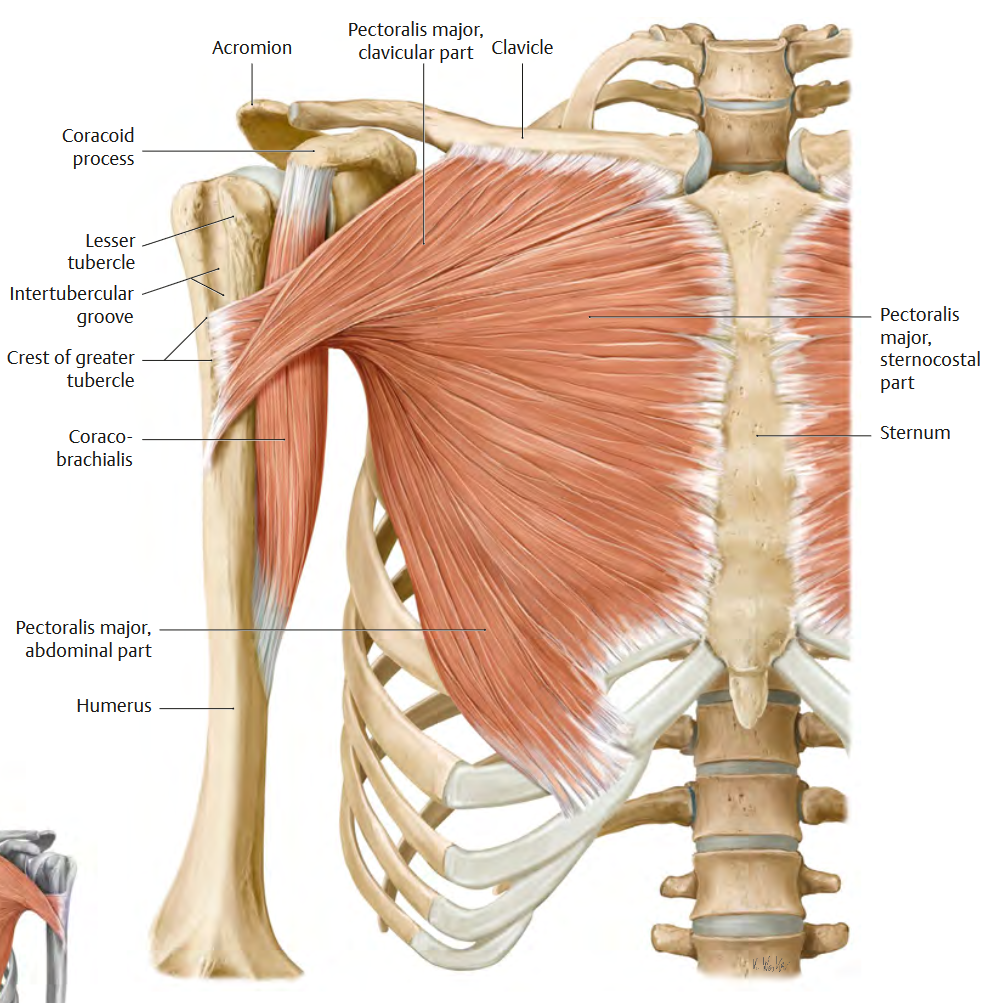
The coracobrachialis can be found deep to the pectoralis major and Anterior Deltoid. The coracobrachialis is anterior to Axillary artery and brachial plexus, so be mindful when palpating and applying pressure8.
Clinician
- Locate pectoralis major (anterior wall of the axilla)8.
- Place one hand on the medial arm, just proximal to the elbow8.
- Place the fingerpads of the other hand into the axilla8.
- Instruct the patient to gently adduct into the non-palpating hand8.
- Palpate the inferior medial edge of the pectoralis major, this will act as a reference point8.
- Dive posterior to pectoralis major into the axilla8.
- Palpate for the “slender” belly of coracobrachialis8.
- Active GHJ adduction should cause it to contract8.
Checklist
- Is the muscle in the medial arm8?
- Is it posterior to pectoralis major8?
- Can you strum along the posterior belly8?
Manual Muscle Test (MMT)
According to Dale Avers10, the coracobrachialis cannot be isolated in a manual muscle test10.
It can, however, be tested alongside other muscles in the shoulder flexion MMT10.
Weakness
Coracobrachialis weakness can be caused by musculocutaneous n. dysfunction6.